Critical Care
You will see by now that the knowledge required for the standard TTE and critical care accreditation is mostly the same. This page shows addtional information you need to know for critical care.
Please note that at the end of the 1st ever BSE exam (which I sat) the BSE president said they were thinking of adding some TOE to the critical care exam. (Just in case you didn't think you had enough to learn.)
Stroke Volume
see echo physics.
PW and CSA of
- LVOT
- RVOT
- Mitral inflow (at annulus)
Fluid responsiveness
IVC
IVC size is correlated to CVP/RAP as above (for spont breathing)
In controlled ventilation IVC will expand in inspiration (as venous return is reduced) and reduce in expiration (opposite of spont).
Absence of respiratory variation means 90% chance will not be fluid responsive.
>11% variation identifies responders (with SR and TV >8mls/kg).
IVC collapsibility index = max diameter - minimum diameter / mean diameter
x100 to get percentage
LV
Variation in LV stroke area (trace area of LV in PSAX papillary level in systole and diastole and minus systole from diastole - see how this changes with respiration) with respiration shown to predict fluid responsiveness (change >16%). Impractical without appropriate software in machine.
Could perhaps look at variation in LVEDarea with respiration (not sure if this has ever been done).
LVOT
Vmax or VTI variation with respiration of >12% predicts fluid responsiveness
(max - min / mean) x 100
VTI increase of >12% 1min after PLR predicts fluid responsiveness.
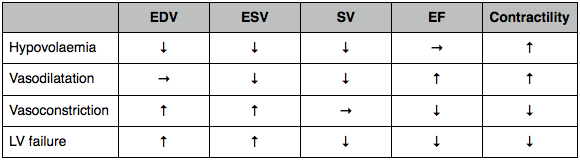
Hypovolaemia
Hyperdynamic LV with reduced LVEDarea (PSAX) (<10cm2) or kissing ventricles (in the absence of hypertrophy/infiltration).
Diastolic dysfunction
Important cause of cardiogenic pulmonary oedema and failure to wean even with reasonable systolic function.
- IHD
- Hypertension
- AS
- Cardiomyopathy
- Sepsis (sepsis induced cardiomyopathy)
- Inotropes (adrenaline). PDE inhibitors (lusitropes) preserve diastolic function better.
- LV can be underfilled despite high filling pressures.
- Optimum filling range narrow (under or over filled easily)
RV dysfunction
- RV volume overload.
- RV pressure overload (ARDS, PE).
- Myocardial contusion (most anterior cardiac chamber).
- Myocardial ischaemia.
- RCA air embolus post cardiac surgery.
Volume overload
RV very compliant so volume can increase with little change in pressure.
If severe volume increase will move over top of Starling curve and start to fail. TR will also develop.
Acute from IV fluid or renal failure.
Chronic from ASD, VSD, severe TR or PR. Chronic volume overload can cause RV hypertrophy and pressure overload. In pure volume overload the RV will not be hypertrophied.
Features of volume overload
Dilated RV
Septum D shaped in diastole (paradoxical motion) going back to normal in systole.
Pressure overload
RV very sensitive to increase in afterload and will quickly result in dilatation and failure if acute (eg PE or ARDS).
If chronic RV will be hypertrophied and will tolerate increased afterload better.
Features of pressure overload
Dilated RV.
Hypertrophied if chronic.
In acute pressure overload (PE or ARDS) will look the same as volume overload with septal flattening in diastole.
If chronic from pulmonary hypertension (recurrent PE, L sided regurg, L heart failure, COPD) RV will be hypertrophied and able to generate very high pressures (>50mmHg). The septum is D shaped in systole (paradoxical motion) going back to normal in diastole.
May open up a PFO and cause R to L shunt and worsen hypoxaemia. In this case, recruitment in ARDS will worsen hypoxaemia by worsening RV failure.
In acute PE, without RV hypertrophy, PA pressures will usually not exceed 50mmHg (unlike chronic overload).
PE
TTE features plus metabolic acidosis (60% mortality) may be an indication for thrombolysis. (ICM 2001). 3% risk significant haemorrhage with thrombolysis.
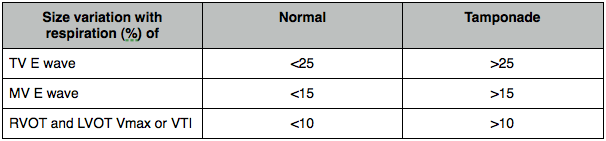
Tamponade
2D and M-mode.
Look for chamber collapse in diastole.
RA then RVOT then whole RV then LA then LV.
RAP will be high so IVC dilated with little or no respiratory variation.
PW
Assess RV and LV inflow in A4C. Inspiration increases flow of blood into R heart (sucks it in) and reduced flow into L heart (pulm vessels expand). This is exaggerated in tamponade (pulsus paradoxus). Remember that this is the opposite if positive pressure ventilation. Measure max and minimum E wave velocities for each valve.
Assess outflow of RVOT and LVOT by measuring Vmax and/or VTI.